Is Intermittent Fasting “Officially” Over?: A Dietitian Reads the Fine Print

A watch on a clean table alongside a colorful, whole-food meal.
If you’ve spent any time on nutrition social media this week, you’ve probably seen the headline: “A new Cochrane review says intermittent fasting is no better than any other diet.” Cue the hot takes, the “TOLD you so” crowd, and approximately 47 confused DMs asking whether to abandon the 16:8.
Here’s the thing: I read the full review—and the broader peer-reviewed literature surrounding it—and the truth is more interesting than any headline can capture. Yes, this review is important and worth taking seriously. But “no better than dietary advice” is not the same as “doesn’t work.” As always, the details are where the story actually lives.
Let’s dig in.
First: What Did the Cochrane Review Actually Find?

Close-up of a researcher reviewing a scientific data on a tablet.
The Cochrane Collaboration publishes what are considered the highest-quality systematic reviews in health research. Rather than relying on a single study, a Cochrane review identifies every rigorous trial on a topic, critically evaluates each one, and combines the results to reach an overall conclusion—essentially the scientific community’s way of getting a consensus answer rather than cherry-picking the studies that agree with a preferred outcome.
Published in February 2026, the Garegnani et al. review1 pooled data from 22 randomized controlled trials involving 1,995 participants across North America, Australia, China, and Europe, with evidence current through November 2024. Participants in these studies were adults with overweight or obesity, and the interventions compared intermittent fasting against conventional dietary advice, no intervention, or a waitlist control.
The Main Findings
Compared to traditional dietary guidance—such as calorie restriction or structured changes to food quality—intermittent fasting produced little to no difference in weight loss. The average additional weight lost with IF was 0.33% of body weight more than conventional dieting, a number so small it carries no real clinical significance. To put that in context: for someone weighing 180 pounds, 0.33% is less than a pound. The 95% confidence interval around that estimate ranged from a small loss to a small gain, meaning the data can’t even rule out the possibility that IF performed slightly worse (Garegnani, et al., 2026).
The review also found no meaningful difference compared to doing nothing or being placed on a waitlist. And across secondary outcomes—quality of life, diabetes markers, and adverse events—the approaches were essentially equivalent.
💡 The Nuanced Nutritionist Take:
The Cochrane finding that IF performs comparably to conventional dietary advice is actually a vote of legitimacy, not a dismissal. These aren’t two radically different results—they’re two equivalent strategies. The headline is not “IF failed.” It’s “IF holds its own.” That distinction matters enormously.
What the Review Missed—And This Is Where It Gets Interesting
Cochrane reviews are rigorous by design, but that rigor comes with built-in constraints. The methodology requires narrow, pre-specified outcome measures, consistent study designs, and sufficient data for meta-analysis. Here are the most significant gaps when you hold this review against the broader literature.
1. The Outcome Set Was Narrow – They Only Looked at the Scale
The review focused almost entirely on weight loss as the primary measure of success. But a substantial and growing body of clinical trial evidence suggests that IF—particularly time-restricted eating (TRE)—produces meaningful improvements in cardiometabolic health markers that are independent of changes in body weight. These include blood pressure, insulin sensitivity, fasting blood glucose, and triglyceride levels (Sun, et al., 2024; Hua, et al., 2025).
Insulin sensitivity refers to how efficiently cells respond to insulin’s signal to absorb glucose from the bloodstream. When insulin sensitivity declines—a condition called insulin resistance—the pancreas compensates by producing more and more insulin to achieve the same effect, a process that over time contributes to prediabetes, type 2 diabetes, and metabolic syndrome. A 2025 meta-analysis of 23 clinical trials found that 16:8 TRE produced statistically significant improvements in fasting blood glucose, insulin resistance, and fasting insulin compared to a control diet (Wong, et al., 2025). None of these effects would appear in a weight-loss-focused review.
2. All IF Protocols Were Lumped Together
The review grouped time-restricted eating, the 5:2 diet, alternate-day fasting, and modified alternate-day fasting under a single “intermittent fasting” label. These protocols differ meaningfully in their physiological mechanisms, caloric impact, behavioral demands, and evidence profiles. Averaging across them is a bit like averaging the effects of a daily brisk walk and competitive marathon training—both qualify as “exercise,” but the comparison hides more than it reveals.
A 2025 network meta-analysis of 56 clinical trials across 16 countries found that modified alternate-day fasting was the top performer for blood pressure and waist circumference reduction, while time-restricted eating showed the strongest effects on fasting blood glucose (Kibret, et al., 2025). Collapsing these into a single category dilutes the signal from protocols that show genuine benefit for specific outcomes.

Two very different IF protocols side-by-side. The 16:8 protocol involves an 8-hour window for eating each day while the 5:2 protocol includes restricted intake for 2 days per week.
3. The Timing of Eating Was Not Considered
Perhaps the most significant scientific gap is that the review treats all eating windows as physiologically equivalent regardless of when in the day they occur. The field of chrononutrition—which studies how meal timing interacts with the body’s internal circadian clock—suggests this assumption is incorrect.
The circadian clock is the body’s internal 24-hour timing system, governing everything from hormone secretion and digestion to insulin sensitivity and fat metabolism (Reytor-Gonzalez, et al., 2025). In practical terms, the body handles the same meal quite differently depending on whether it’s consumed at 8am or 9pm. Insulin sensitivity is naturally highest in the morning and declines across the day; digestive enzyme activity follows a similar rhythm. Early time-restricted eating—placing the eating window in the morning hours, such as 7am to 3pm—aligns food intake with these peak metabolic windows. Late TRE, by contrast, works against them.
A scoping review of 81 human studies concluded that TRE aligned with circadian rhythms produces convergent evidence for improvements in metabolic regulation, insulin sensitivity, gut microbiome composition, and mitochondrial function—some of which appear independently of caloric restriction (Minari, et al., 2025). Early TRE has been shown to improve insulin sensitivity and blood pressure even without significant weight loss (Sutton, et al., 2018).
The Cochrane review’s included studies that neither standardized eating window timing nor reported it consistently, making it impossible to distinguish outcomes from morning eating windows versus evening ones. This is a meaningful methodological limitation given how strongly timing appears to influence results.
4. Adherence Was Averaged Out
The Cochrane review used intent-to-treat analysis, the methodological gold standard in clinical research. Intent-to-treat includes data from everyone who was randomized into a study, regardless of whether they actually followed the protocol. This approach minimizes selection bias and more accurately reflects what happens when a population is simply assigned to a treatment. The tradeoff is that it also captures the outcomes of people who barely tried the intervention alongside those who followed it diligently—which can substantially dilute the observed effect in behavioral interventions like dietary change.
A secondary analysis of an early TRE trial illustrates this clearly. In the full intent-to-treat results, the benefits were modest. When the analysis was restricted to participants who adhered to the protocol at least five days per week throughout the study period, they showed significantly greater reductions in body weight, body fat, heart rate, insulin resistance, and fasting glucose compared to consistent controls (Steger, et al., 2023). In clinical practice, protocol adherence is the central variable—and intent-to-treat analysis, by design, cannot tell us what happens when people actually follow a protocol consistently.
5. Sex Differences Were Not Explored
The review pooled men and women without examining whether outcomes differed by sex, despite growing evidence that women and men respond to fasting protocols differently. Hormonal differences—particularly around the hypothalamic-pituitary axis, which regulates reproductive and stress hormones—mean that the same caloric and temporal restriction can have distinct physiological effects depending on hormonal context.
A 2025 systematic review of 13 clinical trials in women with overweight or obesity found that TRE significantly reduced body weight and fasting insulin without compromising lean body mass—the muscle and structural tissue that drives metabolic rate and physical function. Women in these trials also showed better adherence to TRE than to traditional calorie-restricted diets (Chen, et al., 2025). For women managing perimenopause—the hormonal transition typically beginning in the mid-40s that increases insulin resistance, shifts fat distribution toward the abdomen, and makes sustained caloric restriction harder—these distinctions carry meaningful clinical weight.
What the Broader Research Actually Shows
Nourishing meal prep containers alongside a phone showing a fasting tracker.
Placed in the context of the broader clinical trial literature, the Cochrane review looks less like a definitive verdict and more like one important piece of a complex picture.
Weight Loss and Body Composition
A 2025 meta-analysis of 17 randomized controlled trials found that IF produced a modestly but statistically significant greater reduction in BMI than continuous energy restriction (Alfahl, 2025)—a finding that sits in tension with the Cochrane conclusion but is consistent with the idea that IF is at least an equivalent, and possibly marginally superior, approach to conventional caloric restriction for some outcomes.
More relevant for long-term health than the number on the scale is what happens to body composition during weight loss. Lean body mass—muscle, bone, and connective tissue—is more metabolically active than fat tissue, meaning it contributes more to the body’s resting caloric expenditure. Losing fat while preserving lean mass is the goal of any well-designed weight loss intervention. The women-focused TRE meta-analysis confirmed that TRE achieves meaningful reductions in body weight and fat mass without the lean mass losses that can accompany more aggressive or poorly structured restriction (Chen, et al., 2025).
Blood Sugar and Insulin
This is where the evidence for IF is arguably at its strongest. The 2025 meta-analysis of 23 clinical trials found that 16:8 TRE produced significant reductions in fasting glucose, insulin resistance, and fasting insulin compared to control (Wong, et al., 2025) These improvements in how the body manages blood sugar are clinically meaningful for anyone at elevated risk for type 2 diabetes or currently managing metabolic syndrome—and they appear to reflect the independent effect of meal timing, not just the caloric reduction that often accompanies a compressed eating window.
Cardiovascular Risk Factors
The 56-trial network meta-analysis found that IF protocols significantly reduced body weight, waist circumference, LDL cholesterol, blood pressure, and fasting blood glucose compared to a usual diet (Kibret, et al., 2025). Reductions in waist circumference are particularly meaningful because they reflect decreases in visceral fat—the metabolically active fat stored around the internal organs that is more strongly linked to cardiovascular and metabolic disease risk than overall body weight or subcutaneous fat.
Triglycerides and Cholesterol
An umbrella review of 57 meta-analyses found that TRE modestly reduces triglyceride levels—circulating fat molecules in the blood that, when chronically elevated, raise cardiovascular disease risk—particularly in individuals with overweight (Sun, et al., 2024). Effects on LDL, HDL, and total cholesterol are more variable across protocols and populations, with some evidence that men show more pronounced lipid improvements than women on 16:8 protocols. This variability reinforces the case for protocol selection based on individual health history and goals rather than a one-size-fits-all recommendation.
Cellular Repair and Emerging Evidence
Beyond the outcomes routinely captured in cardiometabolic clinical trials, fasting—particularly longer periodic fasts—activates autophagy, a cellular maintenance process in which the body identifies and breaks down damaged or dysfunctional cell components and recycles them for energy. This process is associated with reduced inflammation, slower cellular aging, and protection against certain chronic diseases (Minari, et al., 2025).The human evidence in this area is in an earlier stage than the cardiometabolic literature, but the mechanistic biology is compelling and active research is ongoing.
There is also emerging clinical evidence that IF positively modulates gut microbiome composition—the community of trillions of bacteria in the digestive tract that influences immunity, inflammation, and metabolic function—in ways that may compound the metabolic benefits of the eating pattern itself (Brasse, et al., 2025).
The Evidence in Summary:
IF is comparable to caloric restriction for weight loss, with the strongest clinical evidence supporting meaningful improvements in blood sugar regulation, insulin sensitivity, blood pressure, and triglycerides—particularly with early, consistent TRE. The cellular and longevity evidence is scientifically interesting but still developing in human research. Cholesterol effects are real but variable.
What This Means for You, Practically Speaking

Enjoying a nourishing meal is empowerment rather than restriction.
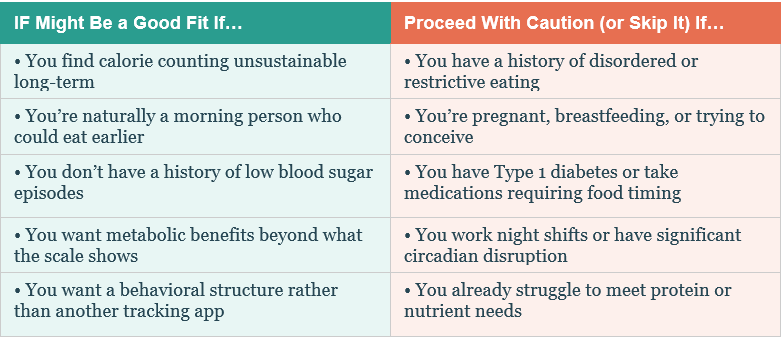
Is IF Right for You? A Quick Framework
The Adherence Argument
One thing the Cochrane review cannot capture is the real-world value of structural simplicity. For many people, the primary barrier to sustained dietary change is not motivation or knowledge—it is the cognitive load of tracking every meal, estimating every portion, and logging every snack day after day. That mental overhead is exhausting, and it’s not a character flaw; it’s a genuine limitation of cognitively demanding behavioral interventions.
Time-restricted eating offers a different kind of structure: a clear daily boundary that removes the need for tracking or macro math. When an eating window helps someone naturally moderate intake, eat more deliberately, and feel less preoccupied with food between meals, that is clinically meaningful—even if its weight loss outcomes are statistically equivalent to a calorie-counting approach in a controlled trial.
Women in TRE trials have shown better adherence than those on traditional calorie-restricted diets, without the lean mass losses that can accompany restriction (Chen, et al., 2025). For women navigating perimenopause, insulin resistance, or stress-related eating patterns, the behavioral sustainability of TRE is a genuinely relevant clinical advantage.
The Nuanced Nutritionist’s Verdict

A balanced plate of lean protein, colorful veggies, whole grains, and healthy fats. A glass of water and a subtle clock in the background.
Here is where I land after reviewing the full evidence landscape:
• IF is not a magic bullet. The Cochrane review is right that it does not reliably outperform conventional dietary advice for weight loss. If weight loss is your only goal, the most important variable is finding an approach you can sustain consistently over time.
• But weight is not the whole story. The cardiometabolic, glycemic, and circadian evidence suggests that IF—especially early TRE—offers meaningful health benefits that a weight-loss-focused analysis will never capture: improved blood sugar regulation, enhanced insulin sensitivity, lower blood pressure, and better triglyceride levels.
• Protocol and timing matter enormously. A 16:8 eating window starting at 7am is a physiologically different intervention from a 16:8 window starting at 4pm and ending at midnight. The research conflates them; the biology does not.
• Adherence is the central variable. Consistently following an early TRE protocol produces meaningful results. Sporadically following any protocol produces modest ones. For many people, the simplicity of time restriction is more sustainable than daily calorie counting—and sustainability determines long-term outcomes.
• Sex-specific considerations are real. Emerging evidence on TRE’s effects on lean mass preservation, insulin sensitivity, and behavioral adherence in women—particularly during perimenopause—makes individualized assessment essential rather than optional.
The Cochrane review is an important corrective to the oversimplified IF hype that has dominated wellness culture. But reading it as “IF is over” fundamentally misreads what the evidence says. The more accurate interpretation: IF is a legitimate, evidence-supported dietary strategy that performs comparably to conventional approaches for weight loss, offers potential advantages for metabolic health that extend well beyond the scale, and deserves a place in the personalized nutrition toolkit—for the right person, with the right protocol, at the right time of day.
That’s pretty nuanced, right?
References
Peer-Reviewed Publications (in order of appearance)
Garegnani LI, Oltra G, Ivaldi D, et al. Intermittent fasting for adults with overweight or obesity. Cochrane Database of Systematic Reviews. 2026;Issue 2. Art. No.: CD015610. DOI: 10.1002/14651858.CD015610.pub2
Sun M-L, Yao W, Wang X-Y, et al. Intermittent fasting and health outcomes: an umbrella review of systematic reviews and meta-analyses of randomised controlled trials. EClinicalMedicine. 2024;70:102519. DOI: 10.1016/j.eclinm.2024.102519
Hua Z, Yang S, Li J, et al. Intermittent fasting for weight management and metabolic health: an updated comprehensive umbrella review of health outcomes. Diabetes Obes Metab. 2025;27(2):920–932. DOI: 10.1111/dom.16092
Wong PS, Wan K, Dai Z, Yu AP, Wong SH, Poon ET. Effect of 8-Hour Time-Restricted Eating (16/8 TRE) on Glucose Metabolism and Lipid Profile in Adults: A Systematic Review and Meta-Analysis. Nutr Rev. Published online December 6, 2025. doi:10.1093/nutrit/nuaf206
Kibret KT, Peeters A, Tegegne TK, Mesfin YM, Nichols M. Intermittent Fasting for the Prevention of Cardiovascular Disease Risks: Systematic Review and Network Meta-Analysis. Curr Nutr Rep. 2025;14(1):93. Published 2025 Jul 24. doi:10.1007/s13668-025-00684-7.
Reytor-González C, Simancas-Racines D, Román-Galeano NM, et al. Chrononutrition and Energy Balance: How Meal Timing and Circadian Rhythms Shape Weight Regulation and Metabolic Health. Nutrients. 2025;17(13):2135. Published 2025 Jun 27. doi:10.3390/nu17132135
Minari TP, Pisani LP. Time-Restricted Eating in Metabolic and Clinical Health: a Current Evidence and Mechanistic Insights. J Nutr. Published online December 30, 2025. doi:10.1016/j.tjnut.2025.101269
Sutton EF, Beyl R, Early KS, Cefalu WT, Ravussin E, Peterson CM. Early Time-Restricted Feeding Improves Insulin Sensitivity, Blood Pressure, and Oxidative Stress Even without Weight Loss in Men with Prediabetes. Cell Metab. 2018;27(6):1212-1221.e3. doi:10.1016/j.cmet.2018.04.010
Steger FL, Jamshed H, Bryan DR, et al. Early time-restricted eating affects weight, metabolic health, mood, and sleep in adherent completers: A secondary analysis. Obesity (Silver Spring). 2023;31 Suppl 1(Suppl 1):96-107. doi:10.1002/oby.23614
Chen S, Zhang X, Kortas J, Liu H. Effects of time-restricted eating on body composition and metabolic parameters in overweight and obese women: a systematic review and meta-analysis. Front Nutr. 2025;12:1664412. Published 2025 Sep 16. doi:10.3389/fnut.2025.1664412
Alfahl SO. Evaluation of the effectiveness of intermittent fasting versus caloric restriction in weight loss and improving cardiometabolic health: A systematic review and meta-analysis. J Taibah Univ Med Sci. 2025;20(2):159-168. Published 2025 Mar 7. doi:10.1016/j.jtumed.2025.02.012
Brasse P, Zerdka J, Staszkiewicz K, et al. Intermittent Fasting: Efficacy, Safety, and Its Impact on Body Weight, Glucose Metabolism, and Gut Microbiota. Cureus. 2025;17(11):e97773. Published 2025 Nov 25. doi:10.7759/cureus.97773
Credible Supplementary Sources
• Cochrane Summary: https://www.cochrane.org/evidence/CD015610_intermittent-fasting-traditional-dietary-advice-or-no-treatment-which-works-better-help-adults
• Academy of Nutrition and Dietetics. Position Statement on Weight Management. J Acad Nutr Diet. 2022.
•.Johns Hopkins Medicine. Intermittent Fasting: What Is It, and How Does It Work? https://www.hopkinsmedicine.org/health/wellness-and-prevention/intermittent-fasting-what-is-it-and-how-does-it-work
Liu D, Huang Y, Huang C, et al. Calorie Restriction with or without Time-Restricted Eating in Weight Loss. N Engl J Med. 2022;386(16):1495-1504. doi:10.1056/NEJMoa2114833
Regmi P, Heilbronn LK. Time-Restricted Eating: Benefits, Mechanisms, and Challenges in Translation. iScience. 2020;23(6):101161. doi:10.1016/j.isci.2020.101161
Elortegui Pascual P, Rolands MR, Eldridge AL, et al. A meta-analysis comparing the effectiveness of alternate day fasting, the 5:2 diet, and time-restricted eating for weight loss. Obesity (Silver Spring). 2023;31 Suppl 1(Suppl 1):9-21. doi:10.1002/oby.23568