Grapefruit: The Fruit That Messes With Your Meds
What furanocoumarins are, why they matter, and what to do about it

Grapefruit, grapefruit juice, and medications on a table with some sprigs of seasoning.
Let’s talk about grapefruit. Beautiful, tart, refreshing, incredibly polarizing at brunch ... and also the only fruit that comes with what amounts to a pharmaceutical warning label.
If you’ve ever been prescribed a statin, a blood pressure medication, or even certain antihistamines, there’s a decent chance your pharmacist has told you to avoid grapefruit. And if you’re like most people, you probably nodded politely while thinking, “Seriously? A fruit?”
Seriously. A fruit. But the story behind why grapefruit causes so many drug interactions is genuinely fascinating, and it’s a great example of how food and pharmacology overlap in ways that most people never think about. So let’s dig in.
The Discovery That Started It All (Completely by Accident)
The grapefruit-drug interaction story begins in 1989 with a research team led by pharmacologist David Bailey. They weren’t studying grapefruit at all. They were testing whether alcohol interacted with the blood pressure medication felodipine, and they used grapefruit juice to mask the taste of ethanol in the study (1).
What they found instead was that grapefruit juice dramatically increased blood levels of felodipine, far beyond what anyone expected. The researchers published their first clinical report on the interaction in 1991, and it opened an entirely new field of food-drug interaction research (1,2).
Since then, more than 85 drugs have been identified as having potential interactions with grapefruit (3). And the list keeps growing. Between 2008 and 2012 alone, the number of drugs known to potentially cause serious adverse effects when combined with grapefruit jumped from 17 to 43.(3)
Meet the Culprits: Furanocoumarins
So, what is it about grapefruit, specifically, that causes all this trouble? The answer comes down to a class of naturally occurring plant compounds called furanocoumarins (fyoo r-oh-koo-muh-rins). The two main players are bergamottin and 6’,7’-dihydroxybergamottin (DHB), both of which are found in relatively high concentrations in grapefruit juice and pulp (4,5).
Furanocoumarins are part of the plant’s natural defense system. They’re not there to sabotage your prescription. Plants produce them as a way to deter herbivores and protect against UV damage. Grapefruit just happens to produce them in quantities that are pharmacologically meaningful for humans.
And here’s where it gets interesting: not all grapefruit varieties contain the same amounts. White grapefruit tends to have higher concentrations of bergamottin and DHB than red or pink varieties. Even within the same variety, furanocoumarin content varies based on growing conditions, storage, and processing methods (4,6). Researchers have even developed new low-furanocoumarin grapefruit cultivars that do not inhibit CYP3A4 at all (5).
The Mechanism: How Grapefruit Breaks Your Drug-Processing Machinery
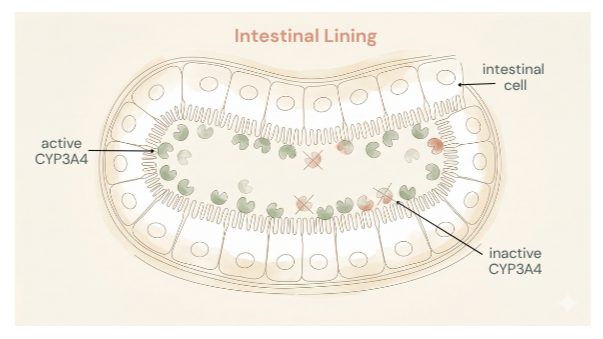
To understand what’s happening, we need to talk about an enzyme called CYP3A4. It belongs to the cytochrome P450 superfamily, and it’s responsible for metabolizing (breaking down) roughly 50% of all marketed drugs (7). That’s an enormous workload for one enzyme. CYP3A4 is found in high concentrations in the cells lining your small intestine and in your liver.
When you take an oral medication, it passes through the wall of your intestine before reaching your bloodstream. During that trip, CYP3A4 in the intestinal cells breaks down a significant portion of the drug before it ever gets to circulate. This is called first-pass metabolism, and for some drugs, it’s substantial. For example, the blood pressure drug felodipine is 100% absorbed from the gut, but its bioavailability is only about 15% after oral administration because CYP3A4 chews through most of it on the way in.(3)
Here’s the problem: furanocoumarins in grapefruit are mechanism-based (irreversible) inhibitors of CYP3A4 (4,7,8). They don’t just temporarily block the enzyme from working; they permanently disable it. The furanocoumarins bind to CYP3A4 and essentially destroy it. The enzyme is done. Finished. Off to the cellular recycling bin.
And because the inhibition is irreversible, your intestinal cells have to manufacture brand-new CYP3A4 enzymes to restore their drug-metabolizing capacity. Research shows it takes about 24 hours to regain 50% of baseline enzyme activity, and it can take a full 72 hours (about three days) for activity to return completely (2,4). That’s why your doctor doesn’t say “just wait a few hours.” Even a single glass of grapefruit juice consumed days before taking certain medications can still influence drug levels.
One study found that CYP3A4 protein levels in the small intestine decreased by 47% within just four hours of consuming grapefruit juice (8). That’s nearly half your drug-metabolizing capacity, gone in an afternoon.
What Happens When CYP3A4 Goes Offline
When CYP3A4 isn’t doing its job in the intestinal wall, more of the drug passes through intact and enters your bloodstream. The result? Higher-than-intended blood levels of the medication. Depending on the drug, this can range from mildly inconvenient to genuinely dangerous.
For a drug like felodipine, research has shown that a single serving of grapefruit juice or one whole grapefruit can cause drug overdose toxicity (2). In a crossover study with buspirone (an anti-anxiety medication), grapefruit juice increased peak plasma concentrations 4.3-fold and the total drug exposure (AUC) 9.2-fold (2). That’s not a small bump; that’s the equivalent of taking roughly nine times your prescribed dose.
The drugs most vulnerable to this interaction tend to share three features: they are taken orally, they normally undergo extensive first-pass metabolism by CYP3A4, and only a small percentage of the original dose makes it into the bloodstream under normal conditions (3). Common drug classes affected include certain statins (simvastatin, lovastatin, atorvastatin), calcium channel blockers (felodipine, nifedipine), immunosuppressants (cyclosporine, tacrolimus), some benzodiazepines (midazolam), and certain antihistamines (3,9).
Potential adverse effects from these boosted drug levels include dangerous heart rhythm changes (torsades de pointes), muscle breakdown (rhabdomyolysis), kidney toxicity, GI bleeding, and respiratory depression (3).
The Plot Twist: Sometimes Grapefruit Makes Drugs LESS Effective
Just when you thought the story was straightforward, grapefruit throws a curveball. For a smaller group of medications, grapefruit does the exact opposite: it decreases how much drug gets into your bloodstream.
This involves a completely different mechanism. Grapefruit juice (along with orange juice and apple juice) can inhibit organic anion-transporting polypeptides (OATPs), which are transporter proteins that help move certain drugs from your intestine into your bloodstream (10,11). When grapefruit blocks these transporters, less drug is absorbed and blood levels drop.
The most well-studied example is fexofenadine (Allegra). Research has shown that a standard glass (300 mL) of grapefruit juice reduced fexofenadine absorption by roughly 42% (11). That’s enough to make the antihistamine noticeably less effective. Other drugs affected by this pathway include certain beta-blockers (acebutolol, celiprolol) and levothyroxine (10).
Importantly, the OATP-blocking mechanism works differently from the CYP3A4 story. The flavonoid naringin appears to be the primary culprit for OATP inhibition, rather than the furanocoumarins.10 And unlike the irreversible CYP3A4 effect that can last for days, OATP inhibition is short-lived, typically resolving within four hours (10). So, separating grapefruit consumption from these medications by about four hours can sidestep the issue.
Not Just Grapefruit: Other Citrus Fruits to Keep on Your Radar

Grapefruit, oranges, limes and other fruits contain furanocoumarins.
Grapefruit gets all the attention, but it’s not the only citrus fruit containing furanocoumarins. Seville oranges (the bitter oranges used in marmalade), limes, pomelos, and tangelos can also contain pharmacologically relevant levels of these compounds (2,9). Regular sweet oranges (navel, Valencia) and their juice do not appear to have the same CYP3A4-inhibiting effect, since they lack significant furanocoumarin content (9).
There’s even a case report in the literature of a patient experiencing tacrolimus toxicity after consuming marmalade that unknowingly contained Seville orange (3). The point isn’t to fear all fruit; it’s to be aware that “grapefruit interaction” is really a “furanocoumarin interaction,” and a handful of other citrus fruits share that chemistry.
So... Can You Eat Grapefruit or Not?
The honest, nuanced answer? It depends.
The interaction between grapefruit and any given drug varies based on the specific medication involved, the individual’s physiology, and even the type and amount of grapefruit consumed. Some experts have pointed out that for the majority of patients, complete avoidance of grapefruit may be unwarranted (6). Others, including Bailey and colleagues, have argued that because the consequences of certain interactions can be severe and are easily preventable, caution is the wiser approach (3).
Here’s the practical takeaway:
Check with your pharmacist. This is genuinely one of the most underused resources in healthcare. Your pharmacist can tell you quickly whether any of your medications interact with grapefruit and how clinically significant the interaction is likely to be.
Read the label. Affected medications typically carry a specific warning about grapefruit on the packaging or in the prescribing information.
Don’t try to use grapefruit to “boost” your medications. Because furanocoumarin content varies so much between grapefruit types, growing conditions, and processing methods, the interaction is not consistent or predictable enough to use therapeutically.6 You could easily undershoot or overshoot, and with narrow-therapeutic-index drugs, that’s risky.
If your medication is affected, know that timing alone may not help for CYP3A4-related interactions. Because the enzyme inhibition is irreversible and takes up to three days to fully recover, simply waiting a few hours between grapefruit and your medication isn’t enough.4 For OATP-related interactions (like fexofenadine), a four-hour gap usually does the trick (10).
Ask about alternatives. In many drug classes, there are options that aren’t significantly affected by grapefruit. For instance, pravastatin and rosuvastatin are generally considered safer choices than simvastatin for statin users who love their grapefruit (3).
The Bottom Line
Grapefruit is a perfectly healthy fruit. It’s rich in vitamin C, fiber, and antioxidants, and there is absolutely nothing wrong with eating it, unless you’re taking specific medications that interact with furanocoumarins. The interaction is real, well-studied, and in some cases, clinically significant. But it’s also manageable with a little awareness and a quick conversation with your pharmacist.
The science here is genuinely cool: a naturally occurring plant defense compound that can irreversibly disable a human drug-metabolizing enzyme, dramatically changing how your body processes medication. It’s one of the best examples of how food and pharmacology intersect in ways that matter for everyday health.
So no, grapefruit isn’t out to get you. But it is worth paying attention to, which is kind of the whole point of nuance.
References
1. Bailey DG, Spence JD, Munoz C, Arnold JMO. Interaction of citrus juices with felodipine and nifedipine. Lancet. 1991;337(8736):268-269. doi:10.1016/0140-6736(91)90872-M https://doi.org/10.1016/0140-6736(91)90872-M
2. Bailey DG, Malcolm J, Arnold O, Spence JD. Grapefruit juice-drug interactions. Br J Clin Pharmacol. 1998;46(2):101-110. doi:10.1046/j.1365-2125.1998.00764.x https://doi.org/10.1046/j.1365-2125.1998.00764.x
3. Bailey DG, Dresser G, Arnold JMO. Grapefruit-medication interactions: Forbidden fruit or avoidable consequences? CMAJ. 2013;185(4):309-316. doi:10.1503/cmaj.120951 https://doi.org/10.1503/cmaj.120951
4. Dayyih WA, Al-Qerem W, Alkhateeb H, et al. Review of grapefruit juice-drugs interactions mediated by intestinal CYP3A4 inhibition. J Appl Pharm Sci. 2024;14(05):059-068. doi:10.7324/JAPS.2024.160197 https://dx.doi.org/10.7324/JAPS.2024.160197
5. Guttman Y, Yedidia I, et al. New grapefruit cultivars exhibit low CYP3A4-inhibition activity. Food Chem Toxicol. 2020;138:111135. doi:10.1016/j.fct.2020.111135 https://doi.org/10.1016/j.fct.2020.111135
6. Hanley MJ, Cancalon P, Widmer WW, Greenblatt DJ. The effect of grapefruit juice on drug disposition. Expert Opin Drug Metab Toxicol. 2011;7(3):267-286. doi:10.1517/17425255.2011.553189 https://doi.org/10.1517/17425255.2011.553189
7. Fuhr LM, Marok FZ, Hanke N, Selzer D, Lehr T. Physiologically based pharmacokinetic modeling of bergamottin and 6,7-dihydroxybergamottin to describe CYP3A4 mediated grapefruit-drug interactions. Clin Pharmacol Ther. 2023;114(2):470-482. doi:10.1002/cpt.2968 https://doi.org/10.1002/cpt.2968
8. Schmiedlin-Ren P, Edwards DJ, Fitzsimmons ME, et al. Mechanisms of enhanced oral availability of CYP3A4 substrates by grapefruit constituents: decreased enterocyte CYP3A4 concentration and mechanism-based inactivation by furanocoumarins. Drug Metab Dispos. 1997;25(11):1228-1233. https://pubmed.ncbi.nlm.nih.gov/9351897/
9. Guo LQ, Yamazoe Y. Inhibition of cytochrome P450 by furanocoumarins in grapefruit juice and herbal medicines. Acta Pharmacol Sin. 2004;25(2):129-136. https://pubmed.ncbi.nlm.nih.gov/14769198/
10. Bailey DG. Fruit juice inhibition of uptake transport: a new type of food-drug interaction. Br J Clin Pharmacol. 2010;70(5):645-655. doi:10.1111/j.1365-2125.2010.03722.x https://doi.org/10.1111/j.1365-2125.2010.03722.x
11. Dresser GK, Kim RB, Bailey DG. Effect of grapefruit juice volume on the reduction of fexofenadine bioavailability: possible role of organic anion transporting polypeptides. Clin Pharmacol Ther. 2005;77(3):170-177. doi:10.1016/j.clpt.2004.10.005 https://doi.org/10.1016/j.clpt.2004.10.005